MRI Siemens Aera 1,5 T
Neurology Report: What I see from your history is that he is a 4 year old male Cocker Spaniel who has an acute onset of generalized seizures starting 4 days ago. There is no previous history of seizures. He has been more lethargic than normal and drinking more than usual. He also wanders aimlessly, standing and opening/closing his mouth and also tilting the head to the right. Blood work results are normal (toxoplasma and neospora with a negative result).
Based on your history, a forebrain disorder is considered. In a dog of his age and breed, I would consider multiple possibilities. It is possible that he is an idiopathic epileptic, but with the pacing and wandering, I worry more about a structural problem. An immune mediated encephalitis, an infectious disease, or even a neoplastic process are considered as well.
To help make a more definitive diagnosis, an MRI of the brain is indicated, just as you pursued.
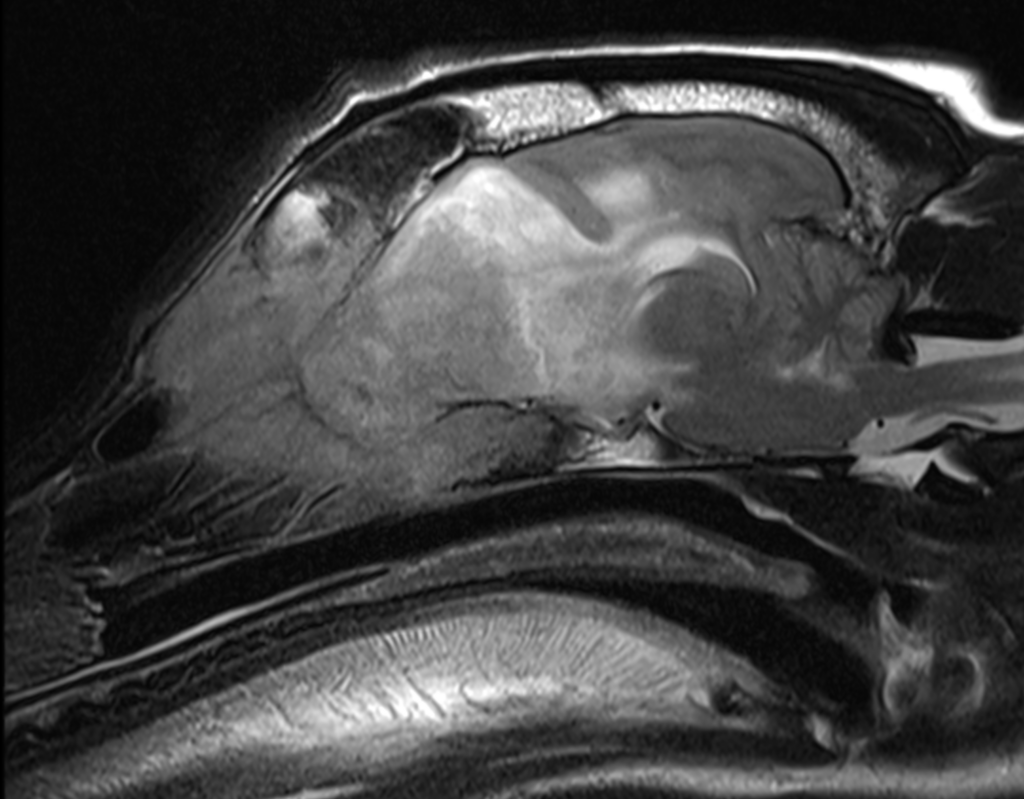
Sag T2
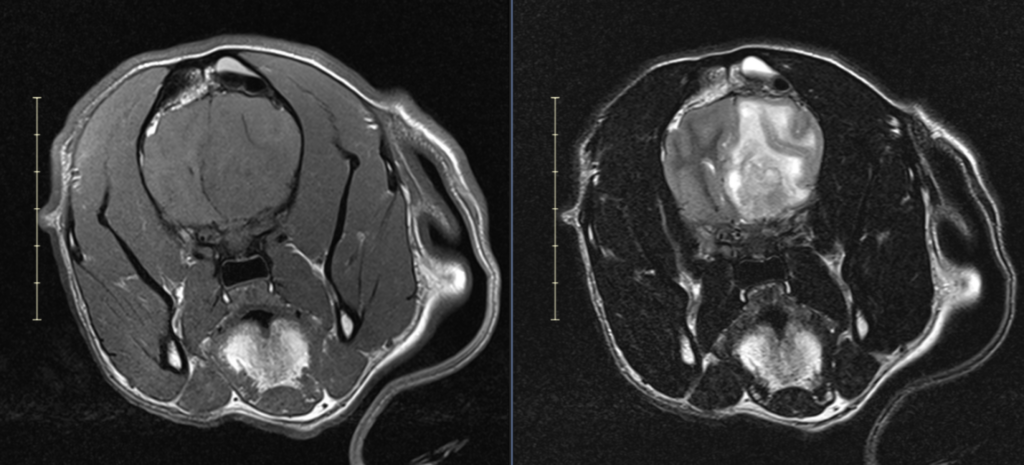
FINDINGS: On review of the MRI, there is a very large, expansile, osteodestructive lesion arising within the right frontal sinus/nasal passage with extension through the cribriform plate and into the brain. The mass is heterogeneously T2 hypo to hyperintense, T1 hypo to isointense and is avidly heterogeneously contrast enhancing. The mass measures 5.3 cm long x 2.3 cm wide x 3.8 cm tall. Surrounding the lesion is a significant amount of T2 and FLAIR hyperintensity within the white matter tracts of the brain. There is moderate right to left brain shift with subfalcine brain herniation and also caudal transtentorial brain herniation. Within the visible portion of the cervical spinal cord, there is marked intraparenchymal T2 hyperintensity.
CONCLUSION: Osteodestructive and infiltrative mass. Presumed neoplastic – esthesioneuroblastoma with nasal and brain components, or a nasal adenocarcinoma with brain invasion. R/O fungal (but MUCH less likely).
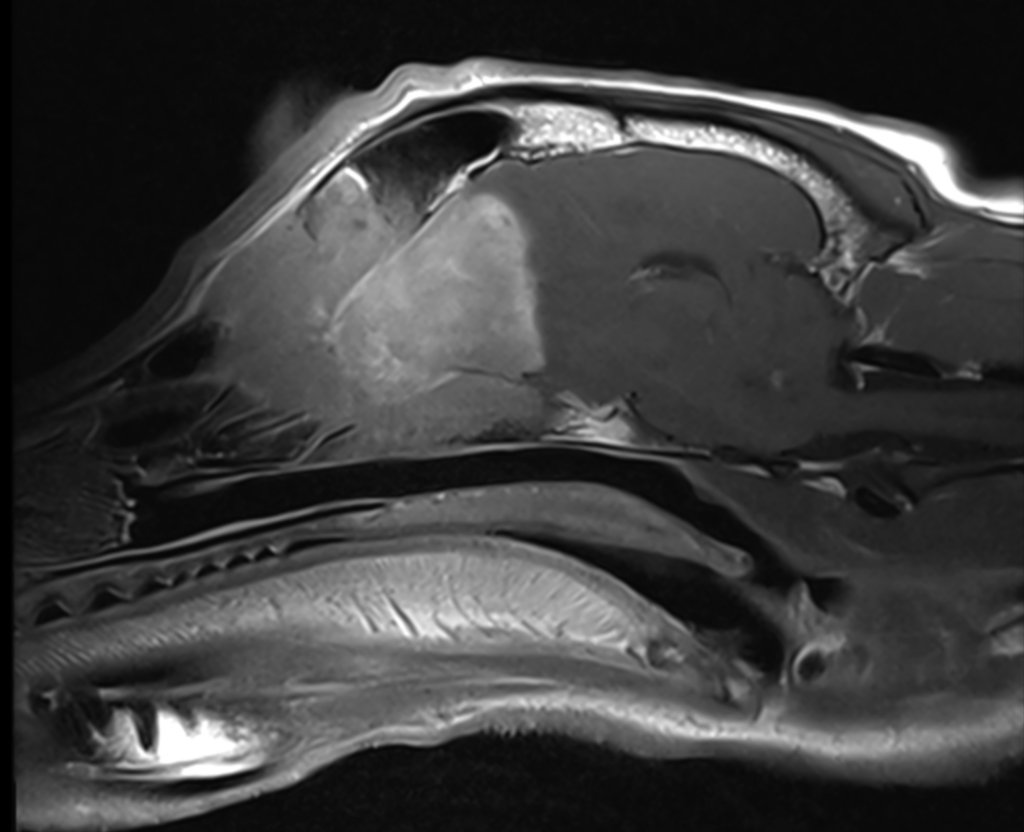
Sag post contrast T1
Cor 0,1 mm post contrast 3D T1
RECOMMENDATIONS: The cause for the seizures is the mass in the nasal passage and brain. I feel that this is most likely a neoplastic process, although a small part of me considers a fungal infection. The first thing to do to help control the seizures would be to reduce the perilesional edema present by using corticosteroids. I would tend to dose higher to help reduce the vasogenic edema faster, using Prednisone at 1mg/kg PO q12h x 14d and then slowly tapering. We would also use an anti-seizure medication, such as Phenobarbital or Levetiracetam (2.5 mg/kg PO q12h or 20 mg/kg PO q8h, respectively). To directly address this mass, you could pursue a surgical therapy, by undergoing a bilateral trans frontal craniotomy to debulk the mass in the frontal sinus, through the cribriform plate, and remove the majority of the mass within the brain. If surgery is pursued, I would still give a few days with high dose prednisone to reduce the edema in the brain and cause less trauma to the normal structures. You can also pursue radiation therapy, but this is a slower treatment and is unlikely to result in a cure. It is important to note that surgery is also unlikely to result in a cure and if this is a nasal adenocarcinoma, they tend to be quite vascular which can lead to intra-operative ischemic infarcts and even hemorrhage to the point of necessitating a blood transfusion. Without direct therapies this mass will continue to grow, invade the brain more, cause more seizures, and will ultimately lead to worsening clinical signs and death.
Reporting Neurologist
Chris Levine, DVM, DACVIM – VetLabs